Using MRI only in prostate cancer radiotherapy workflow
FieldStrength MRI magazine
User experiences - February 2018
Share this article:
MR-only simulation streamlines workflow for prostate cancer radiotherapy
Since March 2017, clinicians in the Department of Oncology and Radiation Therapy at Turku University Hospital (Turku, Finland) have been using Philips MR-only simulation for simulating and planning radiation therapy for their patients with prostate cancer. Featuring the solution’s MRCAT approach, physicists can obtain the needed electron density information for radiotherapy dose calculations, rendering CT unnecessary in the workflow. Moreover, because co-registration of MRI and CT images is not performed in the MR-only workflow, clinicians can avoid registration errors that force margin increases, while exploiting MRI’s exceptional soft tissue visualization to delineate the prostate and organs-at-risk.
“For prostate visualization, the high soft tissue contrast that MRI provides is very important”
Heikki Minn, MD, PhD
Professor and Head of TYKS’s Department of Oncology and Radiotherapy, where he started in 1985. He has previously held research positions at the Academy of Finland, the University of Michigan and Turku PET Centre in Finland. His current interests are head-and-neck and prostate cancer, CNS neoplasms and neuroendocrine tumors.

Jani Keyriläinen, PhD
Medical physicist at TYKS’s Departments of Medical Physics and of Oncology and Radiotherapy. Previous positions at the Helsinki University Central Hospital, and the European Synchrotron Radiation Facility, Grenoble. His current interests are MRI in radiotherapy, small-field dosimetry and dose calculation, quality assurance, and stereotactic and adaptive treatments.
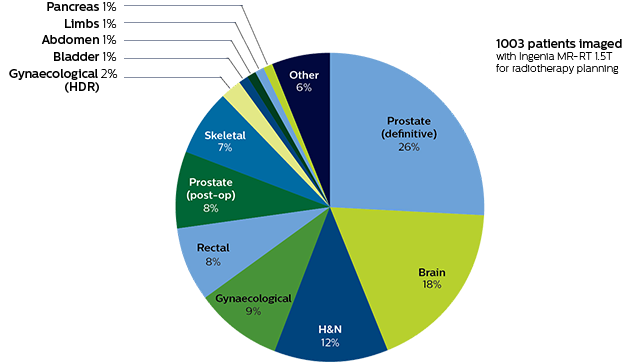
Distribution of patients undergoing MRI for treatment planning at TYKS
January 2016 - October 2017
Exceptional soft tissue imaging with MRI
The radiation therapy department at Turku University Hospital (TYKS) has been home to a Philips Ingenia MR-RT 1.5T since January 2016. This Ingenia is a workhorse for the department, as about 60% of the MRI scans performed are to aid in planning the hospital’s 1,600 radiotherapy patients per year, with cardiac and emergency diagnostic scans making up the balance. Approximately one in five of the radiotherapy cases are prostate cancer patients and for those, MRI simulation is part of the standard clinical care.
In its traditional CT-MRI simulation and planning workflow, Ingenia has been invaluable for its superb, tunable soft-tissue contrast, particularly for planning prostate cancer cases, according to Prof. Heikki Minn, MD, Radiation Oncologist at TYKS.
“For prostate visualization, the high soft tissue contrast that MRI provides is very important,” he says. “Without it, we wouldn’t be able to distinguish the gland from the pelvic muscles and fat surrounding it. That would make it difficult to delineate the prostate and other nearby tissues. We see that our clinical target volume (CTV) for prostate is typically smaller for MRI-based planning, which can help decrease toxicity to the rectum and bladder.
The value of MRI for radiotherapy planning drove the acquisition of the Ingenia for the radiotherapy department. “We wanted to have an MRI in our own department instead of having to use the radiology department’s system, so we can assure our patients get MRI access when it’s feasible for our workflow,” Dr. Minn says.
“Using MR-only simulation and planning would give us a ‘onestop- shop’ workflow for imaging, contouring and planning of radical radiotherapy for patients with prostate cancer,” he says. “Therefore, we began the commissioning process for MR-only simulation immediately in the same month that we began using our Ingenia.”
Distribution of patients undergoing MRI for treatment planning at TYKS
January 2016 - October 2017
"Since March 2017 we have been using MR-only simulation for our prostate patients routinely"
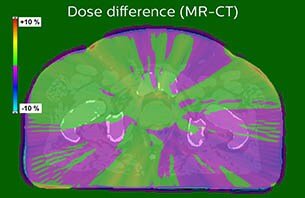
MRCAT dose virtually identical to that of CT-based radiotherapy plans
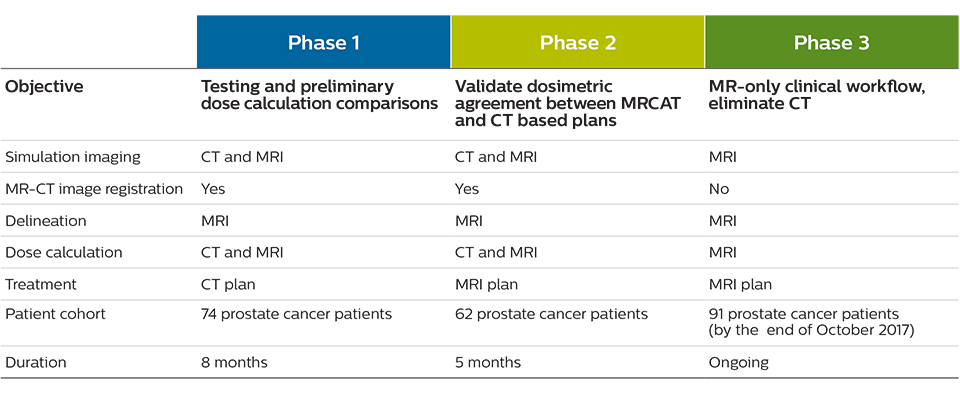
TYKS’s assistant chief physicist Jani Keyriläinen, PhD and medical physicists Sami Suilamo, Lic.Phil., and Pauliina Wright, PhD, led a three-phase commissioning process for MR-only simulation use in prostate radiotherapy, that began in January 2016 and concluded in March 2017. The first phase lasted eight months and consisted of CT-MRI simulation of a control group involving 74 prostate cancer patients.
“These first patients were planned based on CT simulation, but we also did preliminary dose calculation comparisons with both CT and MRI data sets,” Dr. Keyriläinen says. “In the second phase, October 2016 to February 2017, we imaged 62 patients with both CT and MRI, but these patients were planned with the MR images only.
We felt comfortable doing that because we were using thresholds in the dose calculation comparisons – for the planning treatment volumes PTV mean and PTV median – that were set to 2%. We very rarely went over 1% and the average difference in PTV mean values was 0.8% for all 62 patients in the dose comparison. In short, the dose differences between MRCAT- and CT- based radiotherapy plans were minimal. That was a really good sign for us to trust MR-only simulation in the third phase.”
“Since March 2017 we have been using MR-only simulation for our prostate patients routinely,” he says. “So all of the plans are based on MR imaging and calculations. Overall, the commissioning phase went smoothly. Because MR-only simulation is a commercial solution, the learning curve was short, which made commissioning much easier and faster. We didn’t have to start from scratch and find all of the tools ourselves.”
Three-phase commissioning process for MR-only simulation at TYKS
High geometric accuracy of MRI for radiotherapy
In addition to confirming negligible dose differences between CT- and MRI-based simulation, Drs. Minn and Keyriläinen have established that the geometric accuracy of their Ingenia MRRT is high and sufficient for radiotherapy planning. Historically, adoption of MRI in radiotherapy had been hindered by geometric distortions, an issue that has been largely addressed by solutions to correct for gradient distortion and by the use of optimized sequences dedicated for use in radiotherapy. “We have studied this quite carefully, and found that the systeminduced geometrical distortion was less than 1 mm for PTV and organs-at-risk (OAR) volumes in the patient group we studied for this,” Dr. Keyriläinen explains.[1]
Omitting CT in workflow helps save time and eliminates registration errors
With the omission of a CT scan and CT-MR image registration, MR-only simulation has simplified and shortened TYKS’s prostate radiotherapy workflow.
In the TYKS workflow, the initial diagnosis is made with ultrasound-guided biopsy and urological examination. Typically, the MR simulation scan is the first clinical MRI scan the patient receives. There is a strong collaboration with radiologist Terhi Tuokkola, MD, who spends half of her time in the radiotherapy department.
“Her expertise was critical in setting up MR-only simulation. In the beginning, she was instrumental in working with our team of oncologists and MRI physicist on sequence optimization and MR image interpretation. However, her time is limited and our protocol is now a routine process, so getting her diagnostic MRI report for the prostate patients is no longer mandatory,” Dr. Minn observes. “For other clinical areas, such as head-and-neck cancers, that is clearly very different.”
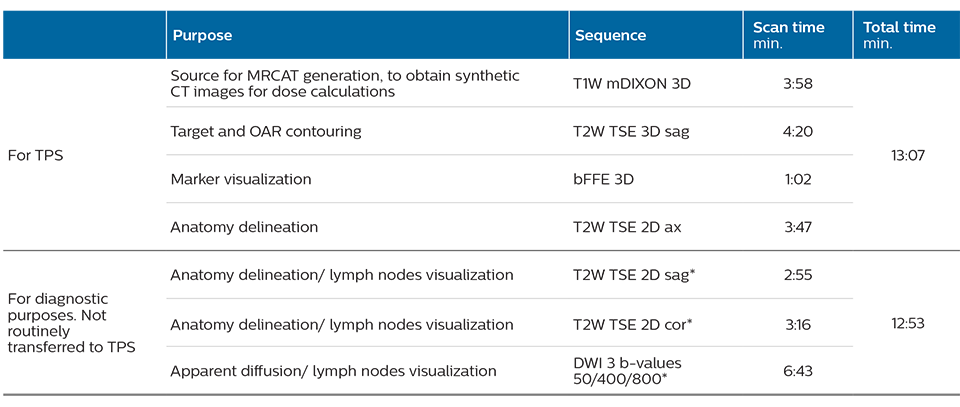
The TYKS MRI examination for generating the images for prostate MR-only simulation includes the standard sequences for MRCAT (Magnetic Resonance for Calculating Attenuation) generation, contouring and fiducial marker visualization. The total scan time for the RT planning sequences is 13 minutes. The ExamCard is customized with additional T2-weighted and DWI sequences for diagnostic purposes which makes total scanning time 26 minutes. The patients are imaged on a flat RT tabletop, using an Anterior MRI coil that is placed on a coil holder to avoid deforming body contours.
The MR images needed for RT planning are exported to the treatment planning system (TPS), where the MRCAT images are handled as a CT image set by the TPS, with no manual postprocessing required. Target and OAR delineation is performed using the T2-weighted images.
TYKS MR-only examination
MRI’s excellent soft tissue visualization facilitates easier delineation
“Delineation is certainly much easier, if not faster, with MR images than with CT images,” Dr. Minn says. “I definitely think the physicians feel more confident because they can see the prostate more clearly and can delineate more consistently. Undoubtedly, this is difficult to measure or assign value, but it is important; inter-physician variability in contouring is decreasing because it is easier to do.”
Using the mDIXON and 3D bFFE images, the RT planner marks the position of the nickel-titanium fiducial markers, and contours are transferred to the digitally reconstructed radiographs (DRRs). Reference image matching is based on these markers. “In the rare cases, where visualization of the fiducial markers fails, we do a CT to confirm their location,” Dr. Keyriläinen notes.
“We think the robustness is getting along quite well. We have less than 5% of prostate cases that are not working with MRCAT and reasons for the failure normally are patient motion, obesity and implants.”
"Delineation is certainly much easier, if not faster, with MR images than with CT-MR images"
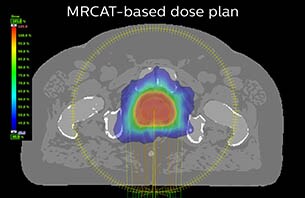
MR-only based planning for prostate cancer radiation therapy treatment
A 77-year-old male with prostate cancer cT3aN0M0, Gleason 8 and PSA 52 μg/L referred to androgen deprivation and radiation therapy with a prescribed dose of 50 Gy to the pelvic lymph node regions and 76 Gy to the prostate.
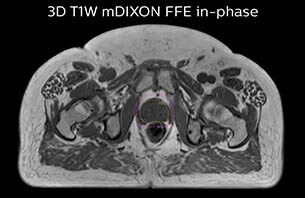
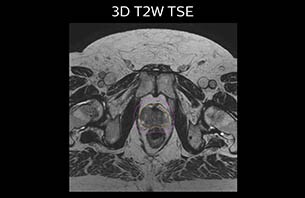
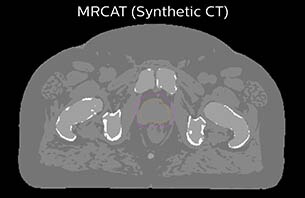
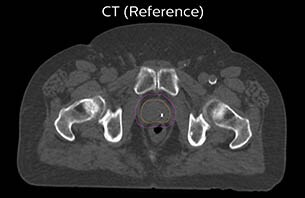
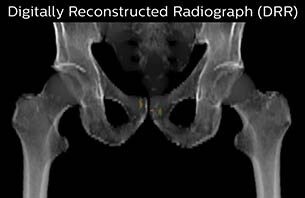
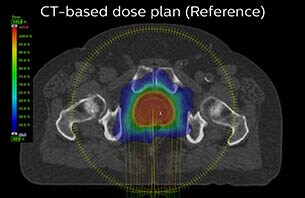
MR-only simulation workflow The 3D T1W FFE mDIXON sequence provides in-phase, water and fat images in one acquisition. Target and organs-at-risk are delineated on the 3D T2W TSE images. Prostate GTV is shown in orange, PTV in purple. The 3D bFFE sequence is used by the planner to mark the position of the fiducial markers (gold anchors) and contours are transferred to the digitally reconstructed radiographs (DRRs).
Based on the 3D T1W mDIXON images, MR-based density maps (MRCAT) are automatically generated. The VMAT (Volumetric Modulated Arc Therapy) plan is generated in TPS, based on MRCAT as primary image set. During the commissioning phase, dosimetric agreement between MRCAT-based and CT-based dose plans was studied and differences in the PTV dose were found to be minimal (<1% for most patients). Average difference in PTV mean values was 0.8% over the study group (n=62).
Philips Ingenia MR-RT 1.5T using the Anterior coil and the integrated Posterior coil.
High staff confidence replaces initial reluctance to use MR-only prostate workflow
TYKS radiation oncologists and physicists adapted quickly to the MR-only simulation for prostate radiotherapy, according to Dr. Minn and Paula Lindholm, MD, PhD, chief radiation oncologist.
“There was some initial reluctance based on limited knowledge about the method, the acquisition technique and different sequences, but now they seem to love the technique, and I think that relates to physician confidence in the soft tissue visualization with MRI,” Dr. Minn says.
“In addition, patients like the fact that they don’t have to spend the time and undergo a scan in a second imaging system, and they don’t receive the dose of ionizing radiation that comes with CT. Truly, we don’t see any downsides to MR-only simulation at the moment.”

Turku University Hospital, Turku, Finland

The MR-RT team at Turku University Hospital
Clinicians look forward to more MR-only simulation applications
“We didn’t intend to implement MR-only simulation just for prostate cases,” Dr. Minn says. “We really need this also for brain and soft tissue tumors such as other pelvic cancer, head-and-neck cases, sarcomas. Clearly, our use of MR-only simulation at TYKS is only going to increase in the future. And I see that this vision also lives in the greater community, as we receive many requests from other Nordic sites to consult with us on how to start MR-only simulation.”
"Truly, we don’t see any downsides to MR-only simulation at the moment"
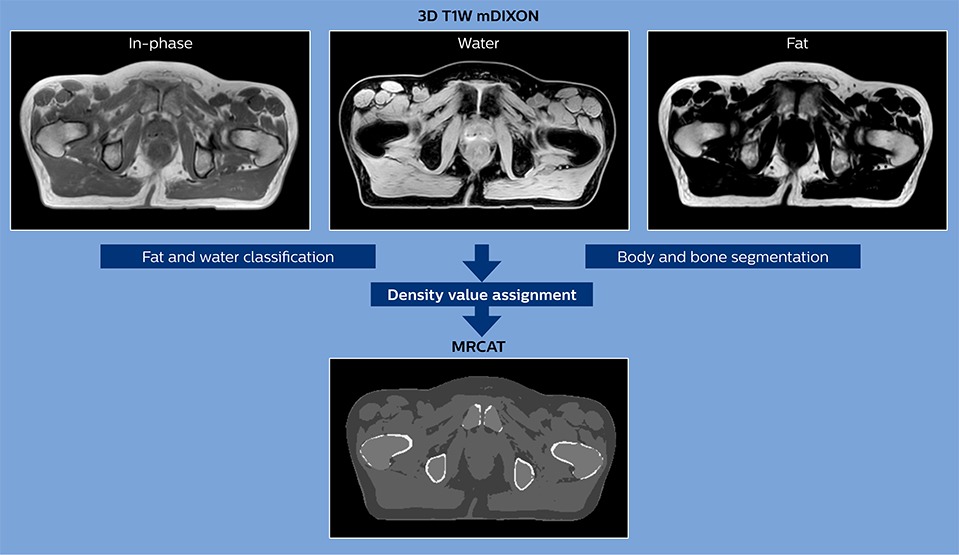
How does MRCAT generation work?
The Philips MRCAT approach for an MR-only based dose planning provides CT-like density information calculated from MR images for dose calculations, as well as high contrast anatomical T2W images for target delineation. [2-3] The MRCAT images with density information are DICOM conform and can be automatically exported to treatment planning systems (TPS) as primary image dataset for dose calculations and to generate MR-based digitally reconstructed radiographs (DRRs).
Electron density information is automatically generated on the MR console from a single T1W mDIXON MRI sequence in two steps:
Several Philips users have described their experiences with MRCAT in peer-reviewed publications. [1,4-5]
References
2. Köhler M, Vaara T, van Grootel M, et al. MR-only simulation for radiotherapy planning – White paper: Philips MRCAT for prostate dose calculations using only MRI data. 2015. 3. Schubert G, Vaara T, et al. Commissioning of MR-only simulation for radiotherapy planning – White paper. www.philips.com/mronlysim. 2017. 4. Christiansen RL, Jensen HR, Brink C. Magnetic resonance only workflow and validation of dose calculations for radiotherapy of prostate cancer. Acta Oncologica, 56(6), 787-791, 2017. 5. Tyagi N, Fontenla S, Zhang J, et al. Dosimetric and workflow evaluation of first commercial synthetic CT software for clinical use in pelvis. Phys Med Biol., 62(8), 2961-2975, 2017.
1. Kemppainen R, Suilamo S, Tuokkola T, et al. Magnetic resonance-only simulation and dose calculation in external beam radiation therapy: a feasibility study for pelvic cancers. Acta Oncologica, 56(6), 2017.
Results from case studies are not predictive of results in other cases. Results in other cases may vary.